I’m with you completely. I do feel for the people who these selfish dummies will invariably infect, but to preserve myself I’ve taken to cynicism.
3 Likes
If you count high-tech developed industrialised states, and look at lab procedures alone, they all should have high accuracy in rPCR testing.
If there are differences, they do not occur because of the PCR itself. Circumstances may vary, of course. Logistics, machinery, availability of testing materials.
But the PCR itself is highly sensitive, and highly accurate.
3 Likes
This is a misleading depiction of the situation. The real point is that all of these tests are dependent on a range of factors - specifically, the severity and stage of the infection. Antigen tests look for protein fragments of the virus, and generally require the infection to be quite widespread through the body and generally will not pick up infections until they are already symptomatic. After the infection is over they will continue to pick up the disease for a while afterwards, by finding remnants of dead virus. Antibody tests look for the body’s immune response to the virus so they are similar to antigen tests.
PCR tests take DNA/RNA from the patient and put them through an amplification step, and then try to match them to the known sequence. The amplification step means they are much more sensitive to the virus if there are very low numbers present, but they still rely on the live virus being present in the sample at all, and if a person is very mildly or early in their infection there just isn’t a lot of virus around. If the body is successful in fighting off the virus, the amount of live virus reduces, so PCR actually increases in false negative rate in later stages of an infection.
In conclusion, you can’t really talk about “accuracy” of tests in isolation without considering exactly who they are testing and when.
In principle you want to use PCR to find infected people early and quarantine them, you use antigen tests to have a rapid determination of if a person with a fever and a cough has covid or something else, and you use antibody tests to try and assess historical cases (though there are some issues with those studies…).

7 Likes
For some, false negatives would be a feature. The higher percentage the better.

3 Likes
I would expect that high just from technique. There is an inherent limitation associated with collecting samples of RNA from the nasal passages, which are loaded with RNases. If a sample sits around long enough before extraction, there’s simply not enough intact viral RNA to replicate with PCR.
9 Likes
Oh God, my heavily Trump supporting community is going to take this the wrong way and will go all out with the stupidity
12 Likes
“We have now proven that, in some people, pre-existing T cell memory against common cold coronaviruses can cross-recognize SARS-CoV-2, down to the exact molecular structures,” said co-author Daniela Weiskopf, a researcher at the La Jolla Institute for Immunology, in a statement released by the research organization. “This could help explain why some people show milder symptoms of disease while others get severely sick.”
13 Likes
Though you’re right about the Trumpers taking this the wrong way, Gov. Cuomo’s response and the plans that I’ve seen are all fairly responsible.
FWIW, I’m in central NY, and we’re going to keep our kiddos home. The district is going to provide a Chromebook and other support. It’s gonna work out ok (I think).
9 Likes
Cuomo is still going to monitor the situation carefully and all districts have to submit their plans with the state. But I have the feeling this going to go poorly in rural & suburban communities
9 Likes
I’m in a rural community in central NY. I’ve been quite impressed with the districts’ efforts. They’ve been upfront about everything I can think of, and they appear prepared for whatever happens next. Good times.
8 Likes
The key is “Done properly.” PCR is notorious for being very technique sensitive. Done well, it should be ~95% accurate or better. Clinically, false negatives are way too high, largely due to poor sample collection technique.
17 Likes
Sorry, should have put the citation int he original post, had to go back and find it.
"Two studies from Wuhan, China, arouse concern about false negative RT-PCR tests in patients with apparent Covid-19 illness. In a preprint, Yang et al. described 213 patients hospitalized with Covid-19, of whom 37 were critically ill.2 They collected 205 throat swabs, 490 nasal swabs, and 142 sputum samples (median, 3 per patient) and used an RT-PCR test approved by the Chinese regulator. In days 1 through 7 after onset of illness, 11% of sputum, 27% of nasal, and 40% of throat samples were deemed falsely negative. Zhao et al. studied 173 hospitalized patients with acute respiratory symptoms and a chest CT “typical” of Covid-19, or SARS-CoV-2 detected in at least one respiratory specimen. Antibody seroconversion was observed in 93%.3 RT-PCR testing of respiratory samples taken on days 1 through 7 of hospitalization were SARS-CoV-2–positive in at least one sample from 67% of patients. Neither study reported using an independent panel, unaware of index-test results, to establish a final diagnosis of Covid-19 illness, which may have biased the researchers toward overestimating sensitivity.
In a preprint systematic review of five studies (not including the Yang and Zhao studies), involving 957 patients (“under suspicion of Covid-19” or with “confirmed cases”), false negatives ranged from 2 to 29%.4 However, the certainty of the evidence was considered very low because of the heterogeneity of sensitivity estimates among the studies, lack of blinding to index-test results in establishing diagnoses, and failure to report key RT-PCR characteristics.4 Taken as a whole, the evidence, while limited, raises concern about frequent false negative RT-PCR results."
20 Likes
Asshole!
17 Likes
That is actually a thing which I couldn’t figure out so far. When I worked in a molecular biology lab, we had to work RNAse free on one bench, and keeping that bench and the samples clean was a painstaking and elaborate process.
And that was pant material. And human RNAse.
Admittedly, that was 20 to 15 years ago, but at least in that period, nothing changed much. The protocols which called for the clean bench could not be adapted, and the process was basically the same all the time, bit with cheaper and more tailored reagents. There is simply no way to do a nasopharyngeal swab without taking massive amounts of RNAse with you, so I figured it must be deactivated, or it doesn’t matter in case of the viral RNA. I hypothesised that the virus particles stay intact, and are lysated in the lab somehow, so the viral RNA is shielded from the RNAse. But so far I haven’t heard anything from someone involved in the actual business of working on tests or developing protocols.
Any ideas yourself? Or @anon29537550?
In general, by the way, I agree that taking and processing the samples is a very probable source of false negatives, and false positives. But 20 to 30 percent false negatives still simply cannot be true. This is far to high in such a deadly game, and without proper citable research on that, I do not believe that number.
Just imagine 30 of 100 people going home after a test, and spreading the virus. R0 would explode.
9 Likes
I’ll try to read that, but I already have the feeling this is one for the specialists to explain the backgrounds and provide context. This would be devastating if true, and hence am deeply suspicious about the number of 20-30%.
I am concerned. (You’ve seen the screenshot above…)
6 Likes
Strictly clinical here. My lab experiences ended in the mid-90’s, so I hope not terribly applicable now. I could hypothesize that the viral transport medium that we stick the swabs in may inactivate RNAse somehow, but I have no clue if that bears any relationship to reality. The nature of getting the sample (esp in peds, which is my area) by its very nature can introduce pretty significant variability. We have switched to OP swabs, as the NP swabs were, umm, “poorly accepted by the patient base” in our situation. I think that might introduce increased reliability issues, based on the NEJM article I cited, but also I hope the techniques have evolved since that article was printed. Again, purely clinical at this point in my life, I can interpret results pretty well, but the nitty gritty of the methods is beyond me.
11 Likes
Former Biolab tech here, my knowledge is 10 years out of date, but 20-30% false negative would be in line with my experience, which is why you do at least 2 pcr tests per sample. Then you would run them again if the results don’t agree.
There are too many ways shit can go wrong from sample taking, to storing, to contamination of workspace or materials, then all the ways you mix the reagents, to lab techs being tired and bored as hell. (I’m so glad not to be working now, it is so easy to skip steps when you have done the same thing day to day for months on end)
I wouldn’t be surprised if shortcuts are taken since reagents are scarce and workload is heavy.
Some of those false negatives may be a timing issue. I know around here there has been a problem with people getting tested too soon after exposure because someone just coughed on them rather than waiting 3+ days later when there would be detectable levels of the virus.
16 Likes
Meanwhile, in the fucking MLB:
Friday’s series opener between the Chicago Cubs and St. Louis Cardinals has been postponed after a St. Louis player tested positive for COVID-19, according to Major League Baseball.
In total, eight Cardinals players have tested positive for the coronavirus since last week.
Emphasis mine. But that wasn’t enough.
The Arizona Interscholastic Association’s executive board
Aka: murderers.
16 Likes
Thing is, it does look as if NY could start cautiously reopening. NY is still doing far too little testing, but consistently finding positivity rates of under 1% in the tests that it is doing. The curve in NY looks like the curve in developed countries, not the one in the US and other dictatorships. (It’s been achieved at a cost - NY now has mandatory 14-day quarantine on persons coming from 36 other states.)
By the way, test positivity looks like the best indicator to monitor: it’s hard to game the positivity rate unless you selectively test the healthy! (The tests can be really crappy for making individual patient decisions and still be statistically informative in the aggregate.) Trump’s ‘just slow down the testing, ok?’, simply makes the metric worse, unless you selectively test only the healthy!
When the base rate falls low enough, the positivity rate simply measures the false positive rate of the test - and I think NY may be close to that, since its new case rate has been running stable at 30-40 cases per million people. That’s surely not good, but it’s more than an order of magnitude down from the peak of nearly 600/million/day. The case fatality rate is down, as well, in the range of 1.5%, down
from ten times that at the peak, when the health care system was overwhelmed.
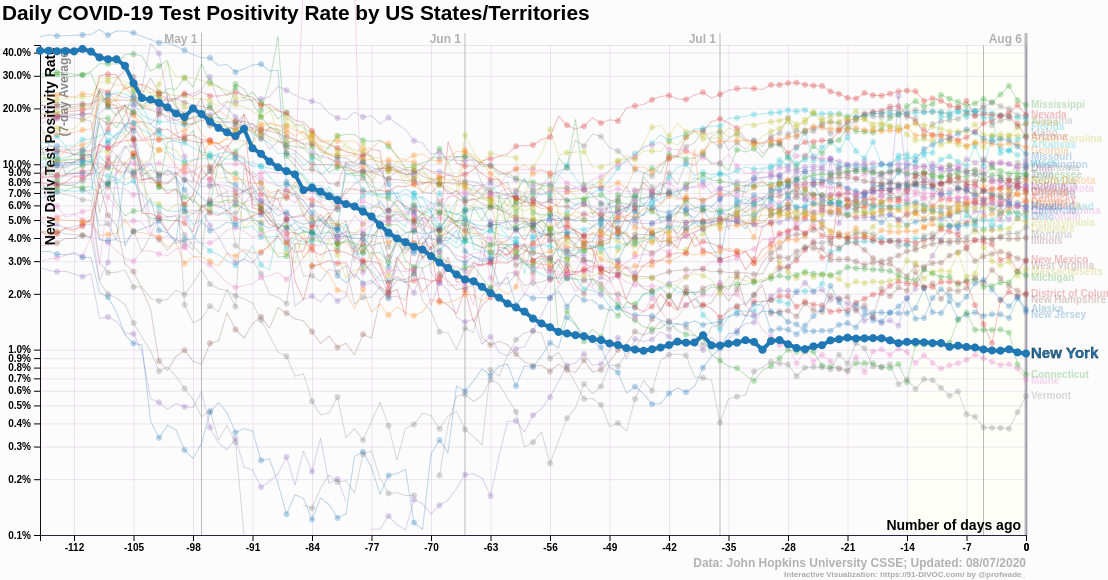
NY has reopened church services under similar restrictions for a month now, and is seeing no indication of increased spread.
And the plans don’t call for full school occupancy. Just that some classes can come in, likely on a shortened schedule to allow for physical distancing in classrooms and aboard buses, with wearing of masks mandatory for all persons in all schools.
Which, as you correctly observe, will be interpreted by right-wingers as ‘NY has given the all-clear!’, and if there is a further resurgence in the virus, it will be the fault of those libtards in NY.
My current nightmare scenario for NY is that some court is going to find that quarantining people coming from out of state is an unconstitutional infringement of the Federal prerogative to regulate interstate commerce, and that NY must let the rest of the country in completely unimpeded. Followed by an inflow of people from the deep-red states coming to infect New Yorkers deliberately, because it’s so totally unfair that New York’s numbers should look so much better than those states. I think it would take relatively few out-of-state Karens to put the situation totally out of control again, if NY’s regulators hands are tied.
I never imagined that the Second Civil War would be fought with biological weapons.
13 Likes